Evaluation of atrial septal defect by cardiac magnetic resonance imaging
Alexios S. Antonopoulos1, Eva Nyktari1, Raad H Mohiaddin1,2
1CMR Unit Royal Brompton Hospital, London UK
2National Heart and Lung Institute, Imperial College London
Clinical Presentation:
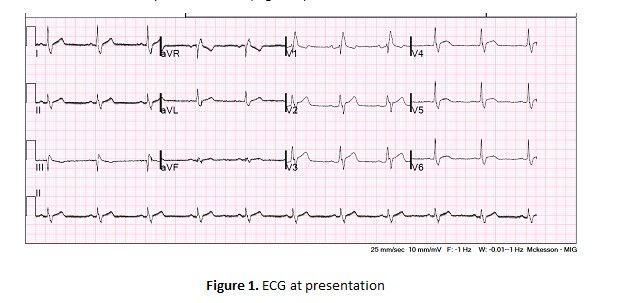
A 66-year-old male presented with symptoms of shortness of breath on exertion. He had a past medical history of paroxysmal atrial fibrillation, hypertension, and dyslipidaemia. His ECG revealed sinus rhythm and RBBB (Figure 1).
The initial transthoracic echocardiography study showed a severely dilated right ventricle with normal systolic function and evidence of pulmonary hypertension. Right atrium was also severely dilated but there was no evidence of a shunt (Videos 1 & 2). The patient was referred to the Pulmonary Hypertension team for further management and the patient was referred for CMR as part of the pulmonary hypertension work up.
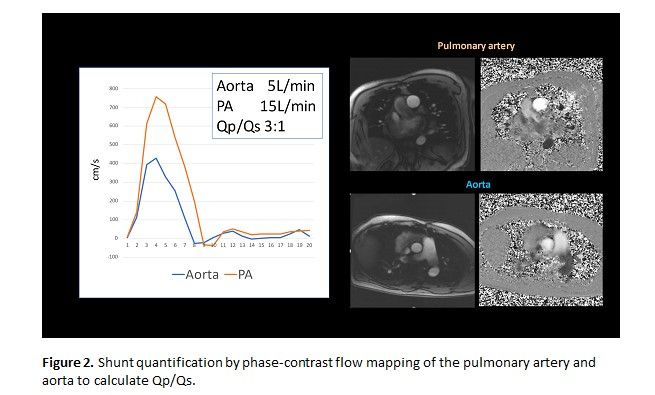
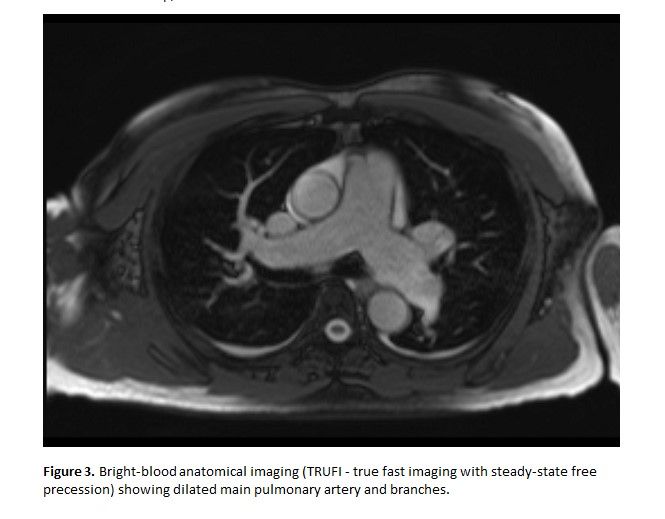
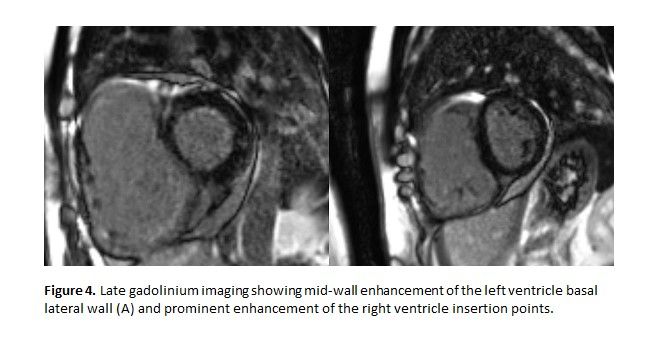
CMR Findings: CMR revealed an unusually located large secundum atrial defect (ASD) at the lower posterior part of the atrial septum measuring ~25x27mm with significant left-to-right shunt (Qp:Qs~3:1, Figure 2 & Video 3). The pulmonary veins were dilated but drained normally into the left atrium. The right ventricle was severely dilated (end-diastolic volume 467mL, 234ml/m2) with normal ejection fraction (RVEF 53%), while there was systolic and diastolic septal flattening suggestive of RV volume and pressure overload with mild RVH (Videos 4-6). The pulmonary branches were dilated (MPA 34mm, RPA 26mm, LPA 31mm, Figure 3). The left ventricle had normal volumes and ejection fraction. The gadolinium study showed subtle mid-wall enhancement of the basal-mid lateral wall and prominent late gadolinium enhancement of the RV insertion points in keeping with pulmonary hypertension (Figure 4). Based on these findings the patient was scheduled for surgical closure of the ASD.
Video 1: Transthoracic echocardiography (sub-costal view) showing a severely dilated right atrium.
Video 2. Subcostal view and doppler imaging showing no flow across the inter-atrial septum
Video 3. Balanced steady-state free precession (bSSFP) imaging by cardiac magnetic resonance showing a large atrial secundum defect (ASD). The ASD falls into the category of a large secundum ASD with an atypical position rather than into that of an inferior sinus venosus ASD since it does not override the interatrial septum (see video 3).
Video 4. Balanced steady-state free precession (bSSFP) imaging by cardiac magnetic resonance 4-chamber view showing a severely dilated right ventricle
Video 5. Balanced steady-state free precession (bSSFP) imaging by cardiac magnetic resonance short axis view showing a severely dilated right ventricle with diastolic and systolic septal flattening suggestive of right ventricle volume and pressure overload.
Video 6. Balanced steady-state free precession (bSSFP) imaging by cardiac magnetic resonance right ventricle in and out view showing normal right ventricle systolic function with mild right ventricle hypertrophy (RV free wall)
Discussion
Transthoracic echocardiography remains the cornerstone for the initial evaluation of patients with pulmonary hypertension and/or suspected intra-cardiac shunts. Transoesophageal echocardiography can also be used for a more detailed assessment of the inter-atrial septum and to investigate for possible atrial septal defect (ASD), while 3D echocardiography provides useful visualization of ASD morphology. Cardiac magnetic resonance (CMR) imaging offers an excellent alternative imaging modality for the evaluation of patients with ASD and is included in the latest European guidelines on the management of ASD.1 CMR offers the advantage of detailed assessment of anatomy, function as well as reliable calculation of pulmonary and systemic flows (Qp/Qs) to quantify the severity of a shunt. CMR can be also used to reliably assess RV volumes and function. CMR or even cardiac computed tomography (CCT) are useful modalities for assessing extra-cardiac anatomy in cases of unexplained right chamber dilation; for example for sinus venosus defects (pulmonary vein anatomy and assessment for partial anomalous pulmonary venous connection or persistent left superior vena cava and unroofed left coronary sinus).2 Indeed, CMR/CCT may be superior to TOE for assessment of inferior sinus venosus defects.1 Early detection and surgical treatment of a sinus venosus defect has is important to lower morbidity and mortality risk of these patients. We have previously shown that the diagnostic value of CMR in patients with unexplained RV enlargement.3 A dedicated CMR imaging protocol can be also used to assess ASD rims’ anatomy and interrogate the suitability of the ASD for percutaneous closure. Previous studies report a good agreement between CMR and TOE for rims’ assessment.4 Careful evaluation of anatomy (sizing of the defect, rims’ anatomy ) as well as shunt size are essential in guiding therapeutic management and assess the suitability for percutaneous closure or surgical treatment.
Key Learning Points
⦁ Transthoracic echocardiography is the first-line diagnostic technique for the diagnosis and quantification of atrial septal defects
⦁ Transoesophageal and 3D echocardiography provide useful information on anatomy.
⦁ Cardiac magnetic resonance (CMR) and cardiac computed tomography (CCT) are excellent alternatives for assessing anatomy and especially in the case of inferior sinus venosus defects may be superior to echocardiography.
⦁ CMR offers essential information on shunt quantification (Qp/Qs), defect size, right ventricle dilation and function to guide therapeutic management.
References
1. Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, Diller GP, Lung B, Kluin J, Lang IM, Meijboom F, Moons P, Mulder BJM, Oechslin E, Roos-Hesselink JW, Schwerzmann M, Sondergaard L, Zeppenfeld K and Group ESCSD. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J. 2020.
2. Ganigara M, Tanous D, Celermajer D and Puranik R. The role of cardiac MRI in the diagnosis and management of sinus venosus atrial septal defect. Ann Pediatr Cardiol. 2014;7:160-2.
3. Kafka H and Mohiaddin RH. Cardiac MRI and pulmonary MR angiography of sinus venosus defect and partial anomalous pulmonary venous connection in cause of right undiagnosed ventricular enlargement. AJR American journal of roentgenology. 2009;192:259-66.
4. Teo KS, Disney PJ, Dundon BK, Worthley MI, Brown MA, Sanders P and Worthley SG. Assessment of atrial septal defects in adults comparing cardiovascular magnetic resonance with transoesophageal echocardiography. J Cardiovasc Magn Reson. 2010;12:44.